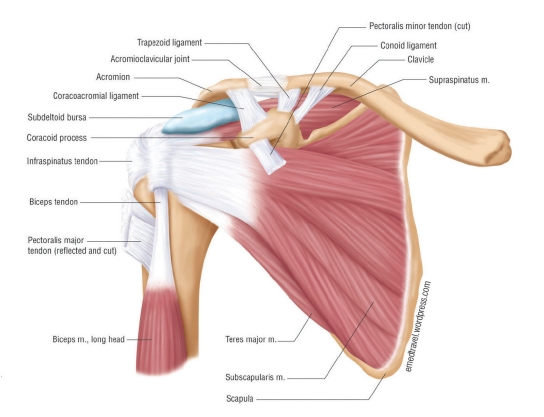
THOUGH NOT ONE of the more common injuries in roller derby, shoulders do see their share of abuse. Whips, bracing, blocks, and impacts on the track provide a special breed of injuries to this part of the body. Let’s start with some basic anatomy. The arm, the humerus, rests in a shallow cup, the fossa, which is part of the shoulder blade, the scapulae. The collar bone, clavicle, and a part of the scapulae called the acromion, join to form the A/C joint. They form a ledge above the humerus and help protect it. The head of the humerus fits into a ring of cartilage called the labrum. Unlike most joints, which are held together predominantly by ligaments, muscle is one of the shoulder’s main sources of support. Ligaments are like filament strapping tape, incredibly strong but not very elastic. Muscles, on the other hand, can contract and relax. This allows the shoulder to have a larger, more sweeping range of motion than almost any other joint. This does come at a cost. The shoulder is not as structurally strong and is more vulnerable to injury. So, what does this mean to you? Most shoulder injuries are due to overuse or trauma. Overuse injuries result from sports/ activities that require a lot of arm use at or above the shoulder level, such as volleyball, racquet sports, and swimming. In derby, trauma is usually caused by a landing on the shoulder. Here is a breakdown of some basic shoulder injuries:
CONTUSION
A few broken blood vessels. The shoulder may be a little black and blue with a little swelling and is tender to the touch. The range of motion is usually full with maybe some stiffness. You’ll be fine. Get back in there, but ice after.
STRAIN
Some muscle fibers are stretched and even torn. Again, he shoulder may show some bruising and there may be a little more swelling and more tenderness to the touch. Range of motion is usually full with some possible stiffness. The treatment is some rest and ice.
SPRAIN
Now you have stretched and possibly torn muscles and may have torn some of the ligaments. The shoulder may be black and blue, but it is definitely swollen and very tender. The range of motion is going to be limited and painful. You need to see your team athletic trainer or doctor and have this assessed. Usually, you can skate with these first three injuries. No contact until you have the full range of motion.
LABRAL TEAR
The labrum is a cup-shaped cartilage that helps hold the humerus in place. Tears in the labrum can come from impact trauma and overuse. If you feel popping, clicking, or grinding in the shoulder or have a sense of instability, rest it, ice it, and do not skate until it has been checked out.
DISLOCATION – OUCH!
Now you have ripped through the muscle, the ligament, and the labrum. Usually, the arm will dislocate forward and down. The most common mechanism of injury is when the humerus is 90° to the side of the body, the elbow bent to 90° with the hand up. This is the most vulnerable position for the arm. If you are hit from behind or land on the shoulder/arm when it is in this position, the humerus can dislocate. Call paramedics or get the skater to a doctor ASAP if this happens. In the interim, it is best to immobilize the arm where it is with gauze or some elastic wrap and start icing. The skater may find it more comfortable if you place a pillow between the arm and the side of the body. Some skaters with chronic/recurrent dislocations can reduce the dislocation themselves if they can do that, great. Still, they are done for the night until they are cleared to return.
So, let’s say you have torn the labrum, sprained, or even dislocated your shoulder; what now? Once your doctor or trainer has cleared you, you can start working on strengthening. As we noted earlier, the shoulder is held together predominantly by muscle, so strengthening the rotator cuff and biceps is key to rehabbing most shoulder injuries. Internal and external rotation exercises can be performed with free weights, cable weights, and elastic bands. Here are the basics. Start with a weight or resistance that you can do with slight effort and move up. Internal rotation is about twice as strong as external rotation, so adjust the weight/resistance accordingly. When doing external rotation exercises, keep the elbow tucked against the side of the body. Also, do bicep curls with the arm coming up from the front of the stomach up to the front of the chest. The motion of a whip, with the arm out to the side, reaching back, and externally rotated (palm up) places the shoulder in a position vulnerable to a repeat of the dislocation. If you have experienced a sprain, a labral tear or a dislocation, have your doctor/trainer assess the shoulder to see if it is strong and stable enough to handle this move.
A/C JOINT SPRAIN
The last injury we will cover is the A/C joint sprain. The acromion and the clavicle join to form the ledge over the humerus and protect the arm from the top. If you land hard on the shoulder and do not fracture the clavicle, the ligaments that hold these bones together may tear. A/C tears are graded 1, 2 and 3, with 1 being a slight tear with little or no movement in the joint and 3 being a complete rupture. So, what do you do for an A/C joint tear?
Given that there are no muscles to strengthen to help support this joint, many doctors say ice it and rest, and beyond that, nothing. Surgery may be indicated in rare cases. In the case of fracture, you may see a deformity in the clavicle. What kind of deformity? Look at both clavicles; it should be pretty obvious if fractured and displaced. Wrap it or put the arm in a sling, ice it and get the skater off to the doctor. Entire books and practices are devoted to diagnosing and treating the shoulder. I hope this informative overview encourages you to learn a little more about these injuries and their care.
Like what we do? Consider chipping in a few bucks.